
Course Content
-
0 / 6
What is ABSR
-
TH: Could ABSR also be called something else?

-
TH: The 7x7 Layers of ABSR
-
HH: ABSR for Anxiety and Stress-related Disorders - Theory (Merkurstab 2023)
-
TH: ABSR for Anxiety, Stress and Trauma - Practice (Merkurstab 2024)
-
HH: Nervousness and Fear (anthrosana 2018)
-
TH/HH: The Impulse of High Sensitivity
-
-
0 / 5
Field Reports
-
0 / 4
Research
-
0 / 5
Training and Handouts
-
0 / 5
ABSR and High Sensitivity
-
0 / 4
Literature
-
0 / 1
Third Party Articles on ABSR
IKIM 2024: ABSR Stress Release

Frontiers in Psychology
Activity-based mindfulness: large-scale assessment of an online program on perceived stress and mindfulness
Eliane Timm (1), Yobina Melanie Ko (1), Theodor Hundhammer (2), Ilana Berlowitz (1†) und Ursula Wolf (1†), 2024.
Front. Psychol. 15:1469316. doi: 10.3389/fpsyg.2024.1469316
(1)Institute of Complementary and Integrative Medicine, Faculty of Medicine, University of Bern, Bern, Switzerland, (2) Eurythmy4you, Nidau, Switzerland, (†)These authors share last authorship

PUBLISHED 15 October 2024 at Front. Psychol. 18:1472562. doi: 10.3389/fnint.2024.1472562
![]()
SUMMARY OF THE RESEARCH ARTICLE
By Theodor Hundhammer, Eurythmy4you, 2024
Activity-based mindfulness: large-scale assessment of an online program on perceived stress and mindfulness
👉 Deutsche Zusammenfassung, German Summary
Abstract
Background: In recent decades, mindfulness has become a central concept in mental health. While current mindfulness-based interventions (MBIs) are often rooted in Asian contemplative traditions, similar practices are also found in integrative medicine systems such as anthroposophic medicine (AM).
Intervention: The Activity-Based Stress Release (ABSR) program incorporates AM as part of an 8-week online intervention, combining mindfulness exercises, behavioural self-observation, and mindful movement. This approach offers an alternative way to cultivate mindfulness, providing diverse methods to address individual differences, clinical demands, or limitations in performing certain practices.
Objective: This study used an observational repeated-measures design to evaluate the feasibility of a large-scale online implementation of the ABSR program, focusing on perceived stress and mindfulness.
Method: Participants enrolled in 37 iterations of the ABSR program. They completed four online surveys using validated stress and mindfulness scales at the beginning, middle, end, and follow-up stages of the intervention.
Results: Of the 830 participants, 53.5% completed at least two surveys, and 22.4% filled in all four surveys . As expected, mindfulness scores increased significantly, while stress scores decreased throughout the intervention. The frequency and duration of self-practice also influenced these outcomes.
Conclusion: This study provides initial indication that the online ABSR program can reduce stress and enhance mindfulness, similar to other MBIs. The findings suggest that this AM-based intervention is adaptable to an online format and offers a novel approach to existing MBIs, addressing the need for diverse methods to suit individual predispositions and clinical requirements.
Outlook: Due to the single-arm design, further controlled studies are needed to confirm these results and to identify which individuals or clinical conditions may benefit most from this method.
Methods
Study Design and Setting
This study was conducted by the Institute of Complementary and Integrative Medicine IKIM in collaboration with Eurythmy4you, an accredited health provider specializing in the ABSR model.
To evaluate the online delivery of ABSR, a longitudinal repeated-measures design was used, with four assessment points to track changes in stress (primary outcome) and mindfulness (secondary outcome).
Participation was fee-based, though rates were kept minimal, with subsidized spaces for those in financial need.
The online study was promoted on the healthcare provider's website, in health magazines, newsletters, clinics offering AM services, medical practices, and on social media.
Intervention
The intervention was an eight-week online ABSR program designed to reduce stress through mindfulness practices drawn from AM. It consisted of 9 weekly 90-minute live online sessions (13.5 hours total) led by a trained ABSR facilitator, with varying amounts of self-practice over 8 weeks.
Facilitators had completed comprehensive ABSR certification, which included personal experience with the program, training lectures, a teaching practicum, and a final assessment involving a written report and presentation.
The intervention was delivered across 37 groups of various sizes and languages (English, German, Russian, Ukrainian, Slovenian, Dutch, Finnish, Chinese, and Spanish).
Each session introduced a new theme (8 modules in total) and the corresponding exercises. Participants were encouraged to practice the exercises daily for at least 15 minutes. In the following session, they could share their experiences and ask questions. Audiovisual materials and a forum were available online, and recordings of missed sessions could be accessed via the web portal.
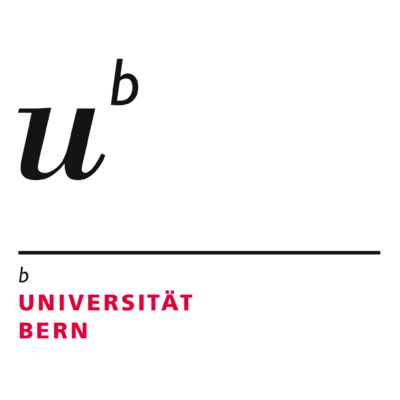
Table 1 outlines the exercises for each module, which were divided into mindful movement exercises (Eurythmy Therapy) and activity-based exercises. The latter required active performance of tasks involving physical or mental effort, despite being performed with a contemplative attitude.
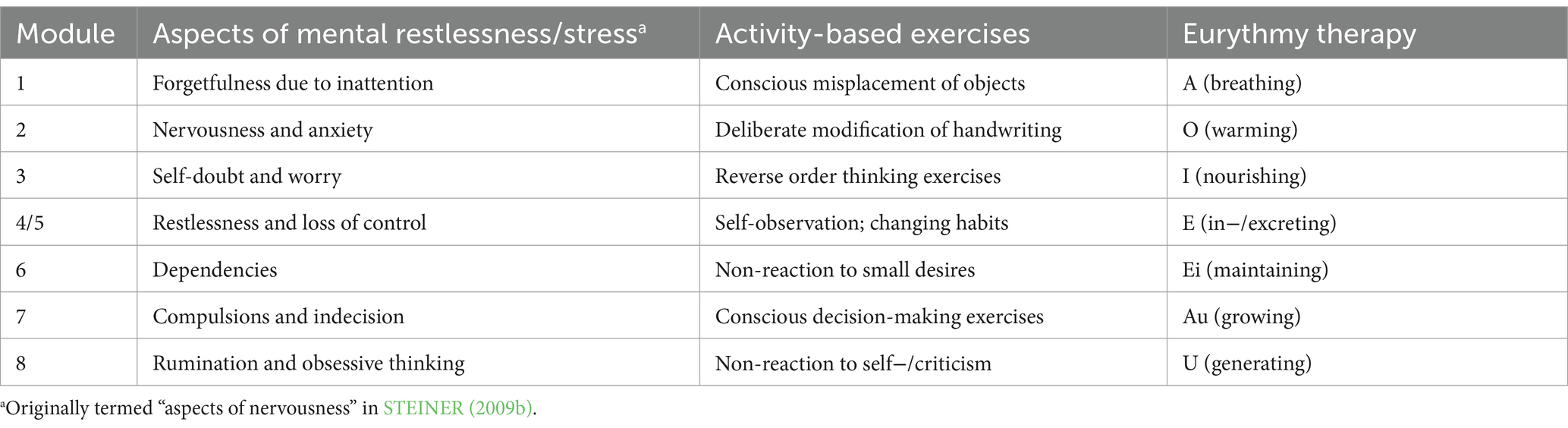
Table 1. ABSR modules, themes, and mindfulness exercises.
Survey
The survey was available in six languages (English, German, Chinese, Spanish, Russian, and Ukrainian). In addition to anonymized demographic information, it included the following measures:
- Stress: The 10-item Perceived Stress Scale (PSS-10) measured stress levels over the past month, with higher scores indicating more stress.
- Mindfulness: The Mindful Attention Awareness Scale (MAAS) assessed mindfulness, with higher scores reflecting greater mindfulness.
- Self-practice and participation: Participants reported how often they practiced the exercises between sessions (days per week) and the daily time spent on them.
Surveys were conducted online at four points: upon registration (up to 3 days before the start of the program; t0), 4 weeks later (t1), at program completion (t2), and 8 weeks after that (t3). Data collection began in September 2023 and concluded in March 2024.
Data Analysis
Participants who agreed to take part and completed at least one survey were included, except for those under 18 or those who participated in more than one cycle of the program.
For analysis, Linear Mixed-Effect Models (LMM) were used as this method handles variations in the target variable over time and produces unbiased estimates even with substantial missing data, a common challenge in online longitudinal studies.
To examine, whether the frequency and duration of self-practice affected outcomes, one-way ANOVAs were conducted, testing if participants who practiced more frequently or for longer durations showed significant differences in stress and mindfulness levels compared to those with less practice.
Results
Characteristics of the Sample
- 1,155 individuals registered in the 37 implementations of the program (English-language implementations had n = 130 registrations, German: n = 259, Chinese: n = 264, Russian: n = 183, Ukrainian: n = 200, Spanish: n = 19, Finnish: n = 33, Dutch: n = 17, and Slovenian: n = 50)
- 830 agreed to participate in the study and filled in the minimally required first survey, as per inclusion criteria (full sample, N = 830).
- 444 (53.5%) filled in at least two surveys
- 186 (22.4%) filled in all four surveys.
Table 2 shows the full sample’s demographic characteristics and language in which the surveys were filled in. The majority of participants were middle aged, female, and of a European context.
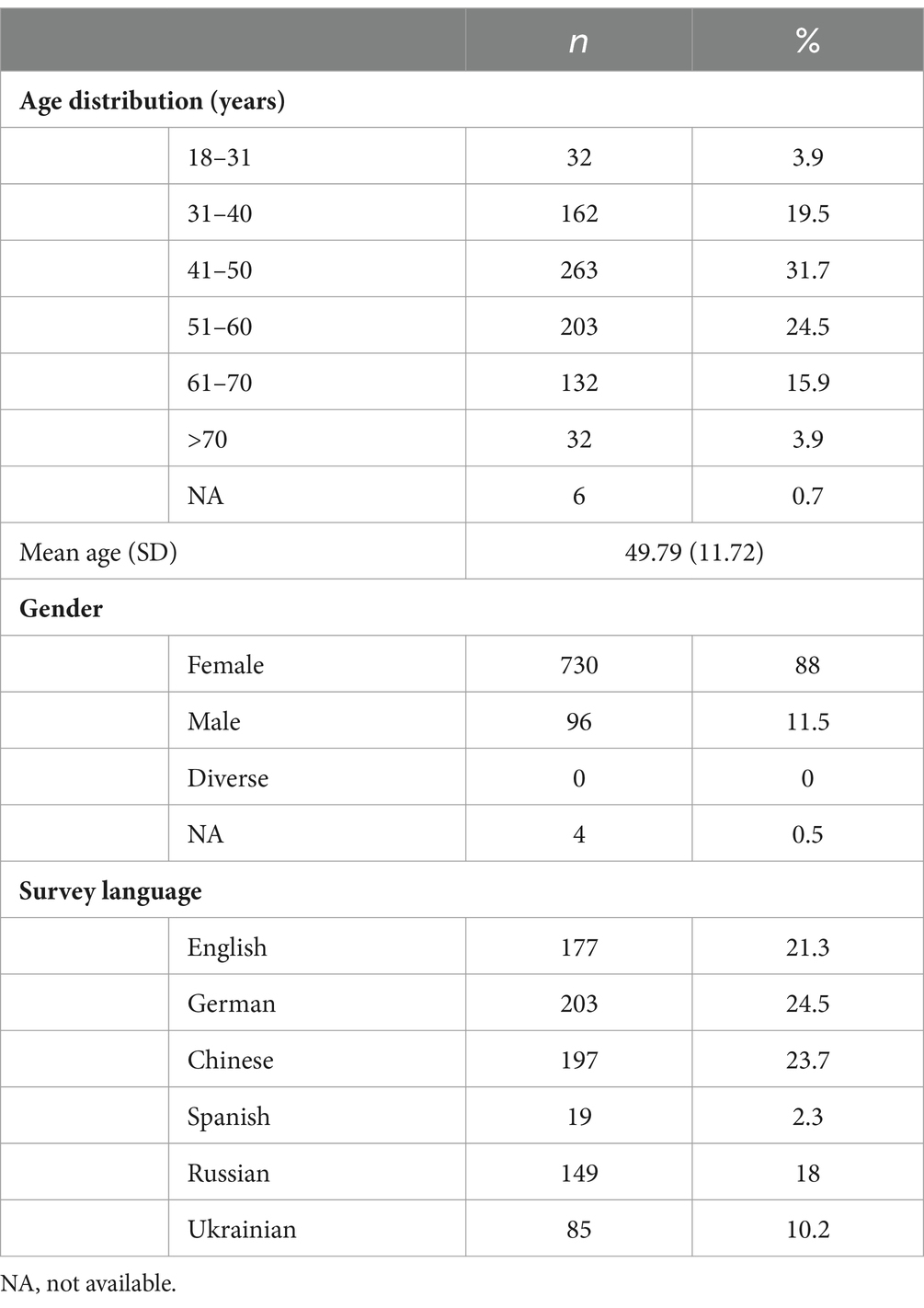
Table 2. Sample characteristics
Baseline
Table 3 presents the sample's stress and mindfulness levels from time point t0 to t3. At t0 (baseline), the Perceived Stress Scale (PSS-10) indicated moderate stress, higher than typical levels for healthy adults, while the Mindful Attention Awareness Scale (MAAS) score was slightly below average compared to general population norms.

Table 3. Self-reported stress and mindfulness per assessment time
Perceived Stress
Changes in self-reported stress over the course of the study, controlled for age, sex, and survey language, can be found in Figure 2. Perceived Stress Scores PSS 10 decreased continuously from t0 to t2 and showed a non-significant small increase again at follow up. All estimates (t1, t2, t3) were significant relative to t0 at p < 0.001.The large F-value, very low p-value, and considerable effect size all support the conclusion that the intervention was effective in decreasing stress among the participants.
Figure 2. LMM model estimated marginal means for perceived stress over time (p < 0.001).
All estimates (t1, t2, t3) were significant relative to t0 at p < 0.001; ***p < 0.001, **p < 0.01, *p < 0.05.
F(3, 902) = 123.969, p < 0.001; effect size ηp2 = 0.28.
Influence of Self Practice on Perceived Stress
Table 4 shows the average frequency and duration of self-practice per time period.
Frequency: Participants on average practiced both types of exercises 2-3 days per week at t1 and t2, dropping to 1-2 days at t3. At t1, t2 and t3, eurythmy-based exercises were practiced slightly more frequently compared to activity-based exercises.
Duration: The average practice time was between 11-20 minutes for both exercise types at t1 and t2, decreasing slightly at t3. Eurythmy-based exercises consistently show longer durations across all time points compared to activity-based exercises.
Both exercise types, eurythmy-based exercises and activity-based exercises, show a similar frequency and duration at t1 and t2, and decrease into t3.

Table 4. Self-practice times: mean frequency and duration.
ANOVA results showed that the frequency and duration of both eurythmy-based and activity-based exercises significantly impacted perceived stress. More frequent practice of both exercise types was associated with lower stress at all time points (t1, t2, t3), while longer practice durations were linked to lower stress at t1 and t2.
For activity-based mindfulness exercises, PSS-10 scores were significantly lower with more days of practice in the weeks preceding assessments at t1 (F(3, 361) = 8.357, p < 0.001), t2 (F(3, 365) = 9.702, p < 0.001), and t3 (F(3, 275) = 4.651, p = 0.003). Longer self-practice durations also significantly reduced stress at t1 (F(4, 360) = 6.479, p < 0.001) and t2 (F(4, 364) = 3.949, p = 0.004).
For eurythmy exercises, stress scores were significantly lower with more frequent practice during the weeks before t1 (F(3, 361) = 5.567, p < 0.001), t2 (F(3, 365) = 10.18, p < 0.001), and t3 (F(3, 275) = 4.261, p = 0.006). Longer practice durations also had a significant effect at t1 (F(4, 360) = 5.297, p < 0.001) and t2 (F(4, 364) = 3.03, p = 0.018).
Mindfulness
Figure 3 shows a significant increase in mindfulness throughout the intervention (F(3, 871) = 82.530, p < 0.001; effect size ηp² = 0.22), with scores consistently rising from t0 to t3. All estimates at t1, t2, and t3 were significantly higher than t0, with p < 0.001.
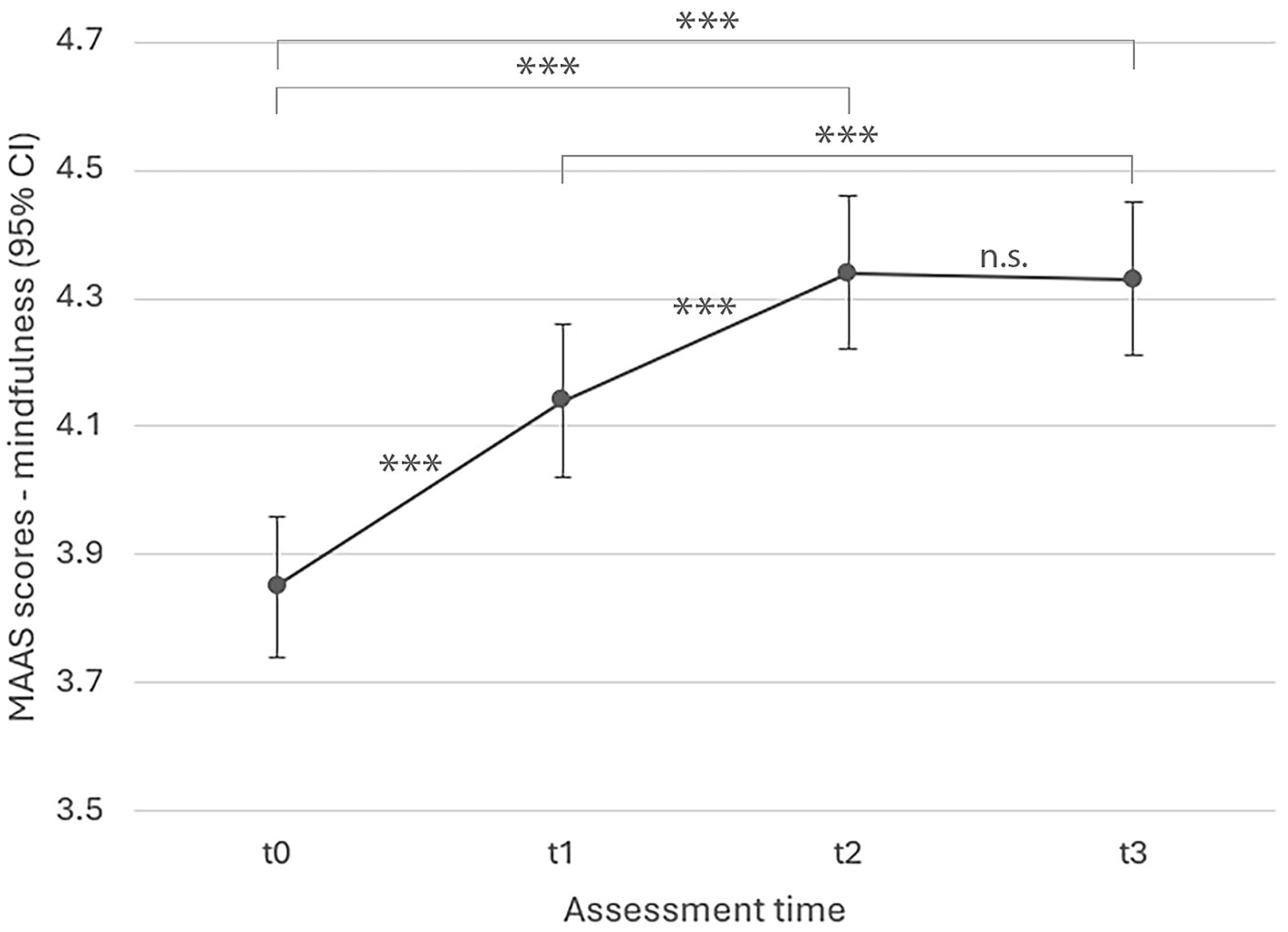
Figure 3. LMM model estimated marginal means for mindfulness over time (p < 0.001).
All estimates (t1, t2, t3) were significant relative to t0 at p < 0.001; ***p < 0.001, **p < 0.01, *p < 0.05.
Discussion
The study evaluated an eight-week online MBI incorporating mindfulness practices from AM (ABSR and Eurythmy), using an observational repeated measures design with a large sample of healthy adults (N = 830).
As expected, self-reported stress significantly decreased during the intervention, with the most notable pronounced improvement occurring by week four. The lower stress level was maintained until 8 weeks after completion of the programme. This stress reduction aligns with findings from other MBIs, such as MBSR, which target stress in healthy adults.
Mindfulness, as measured by the MAAS, also significantly increased throughout the intervention, with a small, non-significant further increase at the eight-week follow-up. These results suggest that, like traditional MBIs, this intervention cultivates mindfulness, though through different methods.
Large effect sizes were found for both stress reduction and mindfulness improvement, comparable to studies using the PSS-10 and MAAS to assess MBSR (though the interpretation of LMM effect sizes across studies is still debated).
The findings showed that improvements in stress and mindfulness were sustained after eight weeks. However, a slight, non-significant rise in stress at follow-up suggests continued self-practice might help maintain benefits over the long term. Indeed, more frequent and longer self-practice was associated with greater improvements, consistent with other MBI studies linking home practice to better outcomes.
The study provides early evidence for the feasibility and benefits of an online MBI based on AM, expanding the diversity of options within the field of MBIs. The intervention’s successful adaptation to an online format also increases accessibility and affordability.
One particular limitation of the study was the single-arm observational design, which is common in early feasibility studies. Future research should use a randomized-controlled design with longer follow-up periods (e.g., 3, 6, 12, and 36 months).
Survey completion rates declined over time, which is typical of voluntary, anonymous online studies. Most dropouts occurred after the first assessment, which is a typical pattern for online interventions and has also been observed in online MBSR studies.
Future studies should consider strategies to improve completion rates, such as offering incentives or personalised reminders.
Further research is needed to explore whether this MBI is particularly beneficial for certain subgroups. Offering a variety of mindfulness practices is advantageous, but more research is required to determine which practices best suit different individuals.
Future studies should therefore assess a broader range of outcomes and clinical populations to determine for whom this AM-based mindfulness approach is most suitable. This would include assess participants' mental health and diagnoses to identify who benefits most and whether there are groups for whom the intervention may be less appropriate.
Conclusion
evidenceWhile this study provides promising early evidence for the online implementation of this novel MBI based on AM practices, these findings need confirmation through randomized-controlled studies, given the limitations of the observational single-arm design and completion rates.
Nevertheless, this research adds a unique contribution to existing MBIs, highlighting the need for diverse approaches to accommodate individual differences and clinical needs. Future research will help establish which subgroups may particularly benefit from this approach, and whether it may be less suitable for others.
October 2024
Theodor Hundhammer![]()
Footnote: The numbers and letters represent results from statistical tests (Analysis of Variance), used to see if there are significant differences between time points or groups.
-
F(3, 902): This is the F-statistic, a value that tells us how much the groups being compared differ from each other. The numbers in parentheses indicate the degrees of freedom (the numbers that represent how much data we have). In this case, 3 represents the degrees of freedom for the differences between time points, and 902 is for the total number of participants (or data points).
-
p = 0.029: The p-value shows whether the result is statistically significant. A p-value below 0.05 (such as 0.029) means there is a significant difference, and the observed change is unlikely due to chance. If the p-value is higher than 0.05, the difference is considered not statistically significant.
- ηp2 = 0.28: ηp2 (eta-squared) is a specific measure of effect size of the strength of a phenomenon. Values range from 0 to 1. 0.01 is considered a small effect, 0.06 is considered a medium effect, 0.14 is considered a large effect and 1 indicates a perfect effect. ηp2 = 0.28 indicates that the intervention had a very large effect on stress levels, explaining 28% of the variance in stress scores. This suggests that the intervention was not only statistically significant but also practically meaningful in reducing stress.
Further Research
Publications on ABSR research can be found here:
References
Adamson, M. M., Phillips, A., Seenivasan, S., Martinez, J., Grewal, H., Kang, X., et al. (2020). International prevalence and correlates of psychological stress during the global Covid-19 pandemic. Int. J. Environ. Res. Public Health 17:9248. doi: 10.3390/ijerph17249248
Anheyer, D., Leach, M. J., Klose, P., Dobos, G., and Cramer, H. (2019). Mindfulness-based stress reduction for treating chronic headache: a systematic review and meta-analysis. Cephalalgia 39, 544–555. doi: 10.1177/0333102418781795
Atkins, W. L. (2018). Empirical mindfulness: traditional Chinese medicine and mental health in the science and religion dialogue. Zygon 53, 392–408. doi: 10.1111/zygo.12416
Baars, E. W., Koster, E. B., and Verhoef, J. (2017). The contribution of Anthroposophic medicine to self-management: an exploration of concepts, evidence, and patient perspectives. Complement. Med. Res. 24, 225–231. doi: 10.1159/000478981
Baer, R. A. (2003). Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin. Psychol. Sci. Pract. 10, 125–143. doi: 10.1093/clipsy.bpg015
Barajas, S., and Garra, L. (2014). Mindfulness and psychopathology: adaptation of the mindful attention awareness scale (Maas) in a Spanish sample. Clínica y Salud 25, 49–56. doi: 10.1016/S1130-5274(14)70026-X
Bartelme, R. R. (2020). Anthroposophic medicine: a short monograph and narrative review—foundations, Essential Characteristics, scientific basis, safety, effectiveness and misconceptions. Glob. Adv. Health Med. 9:216495612097363. doi: 10.1177/2164956120973634
Bates, D., Mächler, M., Bolker, B., and Walker, S. (2015). Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67, 1–48. doi: 10.18637/jss.v067.i01
Bawa, P. (2016). Retention in online courses: exploring issues and solutions—a literature review. SAGE Open 6:2158244015621777. doi: 10.1177/2158244015621777
Beblo, T., Haehnel, K., Michalak, J., Iffland, B., and Driessen, M. (2024). Integrating mindfulness practice into everyday life after completing a course in mindfulness-based stress reduction. Nord. Psychol., 1–13. doi: 10.1080/19012276.2024.2303432
Berger, B., Bertram, M., Kanitz, J., Pretzer, K., and Seifert, G. (2015). “Like walking into an empty room”: Effects of Eurythmy therapy on stress perception in comparison with a sports intervention from the subjects’ perspective—A qualitative study. Evid. Based Complement. Alternat. Med. 2015:856107. doi: 10.1155/2015/856107
Birnie, K., Speca, M., and Carlson, L. E. (2010). Exploring self-compassion and empathy in the context of mindfulness-based stress reduction (Mbsr). Stress Health 26, 359–371. doi: 10.1002/smi.1305
Bodhi, B. (2012). Comprehensive manual of abhidhamma: The abhidhammattha sangaha : Pariyatti Publishing.
Bowen, D. J., Kreuter, M., Spring, B., Cofta-Woerpel, L., Linnan, L., Weiner, D., et al. (2009). How we design feasibility studies. Am. J. Prev. Med. 36, 452–457. doi: 10.1016/j.amepre.2009.02.002
Brown, K. W., and Kasser, T. (2005). Are psychological and ecological well-being compatible? The role of values, mindfulness, and lifestyle. Soc. Indic. Res. 74, 349–368. doi: 10.1007/s11205-004-8207-8
Brown, K. W., and Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 84, 822–848. doi: 10.1037/0022-3514.84.4.822
Büssing, A., Edelhäuser, F., Weisskircher, A., Fouladbakhsh, J. M., and Heusser, P. (2011). Inner correspondence and peacefulness with practices among participants in Eurythmy therapy and yoga: a validation study. Evid. Based Complement. Alternat. Med. 2011:329023. doi: 10.1155/2011/329023
Carlson, L. E., and Brown, K. W. (2005). Validation of the mindful attention awareness scale in a cancer population. J. Psychosom. Res. 58, 29–33. doi: 10.1016/j.jpsychores.2004.04.366
Chen, S.-Y., Cui, H., Zhou, R.-L., and Jia, Y.-Y. (2012). Revision of mindful attention awareness scale (Maas). Chin. J. Clin. Psych. 20, 148–151.
Chiesa, A., and Serretti, A. (2009). Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. J. Altern. Complement. Med. 15, 593–600. doi: 10.1089/acm.2008.0495
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24, 385–396. doi: 10.2307/2136404
Cullen, M. (2011). Mindfulness-based interventions: an emerging phenomenon. Mindfulness 2, 186–193. doi: 10.1007/s12671-011-0058-1
Dahlin, B. (2009). On the path towards thinking: learning from Martin Heidegger and Rudolf Steiner. Stud. Philos. Educ. 28, 537–554. doi: 10.1007/s11217-009-9147-1
De Abreu Costa, M., D’alò De Oliveira, G. S., Tatton-Ramos, T., Manfro, G. G., and Salum, G. A. (2019). Anxiety and stress-related disorders and mindfulness-based interventions: a systematic review and multilevel Meta-analysis and Meta-regression of multiple outcomes. Mindfulness 10, 996–1005. doi: 10.1007/s12671-018-1058-1
De Paepe, L., Zhu, C., and Depryck, K. (2018). Drop-out, retention, satisfaction and attainment of online learners of Dutch in adult education. Int. J. E Learn. 17, 303–323.
Dobkin, P. L., Irving, J. A., and Amar, S. (2012). For whom may participation in a mindfulness-based stress reduction program be contraindicated? Mindfulness 3, 44–50. doi: 10.1007/s12671-011-0079-9
Davis, D. M., and Hayes, J. A. (2011). What are the benefits of mindfulness? A practice review of psychotherapy-related research. Psychotherapy, 48, 198.
Enkema, M. C., Mcclain, L., Bird, E. R., Halvorson, M. A., and Larimer, M. E. (2020). Associations between mindfulness and mental health outcomes: a systematic review of ecological momentary assessment research. Mindfulness 11, 2455–2469. doi: 10.1007/s12671-020-01442-2
Fish, J., Brimson, J., and Lynch, S. (2016). Mindfulness interventions delivered by technology without facilitator involvement: what research exists and what are the clinical outcomes? Mindfulness 7, 1011–1023. doi: 10.1007/s12671-016-0548-2
Fisher, V., Li, W. W., and Malabu, U. (2023). The effectiveness of mindfulness-based stress reduction (Mbsr) on the mental health, HbA1C, and mindfulness of diabetes patients: a systematic review and meta-analysis of randomised controlled trials. Appl. Psychol. Health Well Being 15, 1733–1749. doi: 10.1111/aphw.12441
Fogaça, L. Z., Portella, C. F. S., Ghelman, R., Abdala, C. V. M., and Schveitzer, M. C. (2021). Mind-body therapies from traditional Chinese medicine: evidence map. Front. Public Health 9:659075. doi: 10.3389/fpubh.2021.659075
Gabrio, A., Plumpton, C., Banerjee, S., and Leurent, B. (2022). Linear mixed models to handle missing at random data in trial-based economic evaluations. Health Econ. 31, 1276–1287. doi: 10.1002/hec.4510
Galante, J., Friedrich, C., Dawson, A. F., Modrego-Alarcón, M., Gebbing, P., Delgado-Suárez, I., et al. (2021a). Mindfulness-based programmes for mental health promotion in adults in nonclinical settings: a systematic review and meta-analysis of randomised controlled trials. PLoS Med. 18:e1003481. doi: 10.1371/journal.pmed.1003481
Galante, J., Stochl, J., Dufour, G., Vainre, M., Wagner, A. P., and Jones, P. B. (2021b). Effectiveness of providing university students with a mindfulness-based intervention to increase resilience to stress: 1-year follow-up of a pragmatic randomised controlled trial. J. Epidemiol. Community Health 75, 151–160. doi: 10.1136/jech-2020-214390
Garland, E. L., Gaylord, S. A., Palsson, O., Faurot, K., Douglas Mann, J., and Whitehead, W. E. (2012). Therapeutic mechanisms of a mindfulness-based treatment for Ibs: effects on visceral sensitivity, catastrophizing, and affective processing of pain sensations. J. Behav. Med. 35, 591–602. doi: 10.1007/s10865-011-9391-z
Gold, P. W. (2015). The organization of the stress system and its dysregulation in depressive illness. Mol. Psychiatry 20, 32–47. doi: 10.1038/mp.2014.163
Goldsmith, E. S., Koffel, E., Ackland, P. E., Hill, J., Landsteiner, A., Miller, W., et al. (2023). Evaluation of implementation strategies for cognitive behavioral therapy (Cbt), acceptance and commitment therapy (act), and mindfulness-based stress reduction (Mbsr): a systematic review. J. Gen. Intern. Med. 38, 2782–2791. doi: 10.1007/s11606-023-08140-4
Golubev, A. (2012). Priroda polnoty soznaniya. Adaptatsiya oprosnika vnimatelnosti i osoznannosti Maas [the nature of mindfulness. Adaptation of an awareness and mindfulness questionnaire]. Bull. Nsu. Psychol. 6, 44–51.
Gravesande, J., Almeida De Oliveira, L., Malik, N., Vrkljan, B., Zheng, R., Gardner, P. M., et al. (2023). Feasibility, usability, and acceptability of online mind–body exercise programs for older adults: a scoping review. J. Integr. Complement. Med. 29, 538–549. doi: 10.1089/jicm.2022.0822
Haas, H. (2017). Salutogenese und achtsamkeitsorientierte anthroposophische Psychotherapie am Beispiel ambulanter Gruppentherapien bei “Nervosität”. Schweizerische Zeitschrift für Ganzheitsmedizin 29, 330–335. doi: 10.1159/000484462
Haas, H., and Hundhammer, T. (2013). Selbsterziehung und der achtgliedrige Pfad - ein Gruppenprogramm. Der Merkurstab. Zeitschrift für Anthroposophische Medizin 66, 496–506. doi: 10.14271/DMS-20232-DE
Hayes, S. C., and Hofmann, S. G. (2021). “Third-wave” cognitive and behavioral therapies and the emergence of a process-based approach to intervention in psychiatry. World Psychiatry 20, 363–375. doi: 10.1002/wps.20884
Hoge, E. A., Bui, E., Mete, M., Dutton, M. A., Baker, A. W., and Simon, N. M. (2023). Mindfulness-based stress reduction vs escitalopram for the treatment of adults with anxiety disorders: a randomized clinical trial. JAMA Psychiatry 80, 13–21. doi: 10.1001/jamapsychiatry.2022.3679
Human Research Act of 2011 (2011). AS 2013 3215, SR 810.30. https://www.fedlex.admin.ch/eli/cc/2013/617/en Federal Council of Switzerland.
Jacobsen, P., Choksi, T., Sawyer, K., Maximen, C., Harding, E., and Richardson, M. (2022). Home practice in mindfulness-based interventions for psychosis groups: a systematic review and qualitative study. BMC Psychol. 10:9. doi: 10.1186/s40359-021-00694-4
Jayawardene, W. P., Lohrmann, D. K., Erbe, R. G., and Torabi, M. R. (2017). Effects of preventive online mindfulness interventions on stress and mindfulness: a meta-analysis of randomized controlled trials. Prev. Med. Rep. 5, 150–159. doi: 10.1016/j.pmedr.2016.11.013
Jensen, J. H., Flachs, E. M., Petersen, K. U., Sejbæk, C. S., Ross, L., Eller, N. H., et al. (2023). Changes in perceived stress during a mindfulness-based stress reduction (MBSR) intervention predicting occupational recovery from work-related stress: A longitudinal study.
Juul, L., Pallesen, K. J., Piet, J., Parsons, C., and Fjorback, L. O. (2018). Effectiveness of mindfulness-based stress reduction in a self-selecting and self-paying community setting. Mindfulness 9, 1288–1298. doi: 10.1007/s12671-017-0873-0
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness : Delta.
Kabat-Zinn, J. (2003a). Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. Sci. Pract. 10, 144–156. doi: 10.1093/clipsy.bpg016
Karami, N., Kazeminia, M., Karami, A., Salimi, Y., Ziapour, A., and Janjani, P. (2023). Global prevalence of depression, anxiety, and stress in cardiac patients: a systematic review and meta-analysis. J. Affect. Disord. 324, 175–189. doi: 10.1016/j.jad.2022.12.055
Khoury, B., Sharma, M., Rush, S. E., and Fournier, C. (2015). Mindfulness-based stress reduction for healthy individuals: a meta-analysis. J. Psychosom. Res. 78, 519–528. doi: 10.1016/j.jpsychores.2015.03.009
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., et al. (2013). Mindfulness-based therapy: a comprehensive meta-analysis. Clinical psychology review. 33, 763–771.
Kienle, G. S., Albonico, H. U., Baars, E., Hamre, H. J., Zimmermann, P., and Kiene, H. (2013). Anthroposophic medicine: an integrative medical system originating in europe. Glob. Adv. Health Med. 2, 20–31. doi: 10.7453/gahmj.2012.087
Kloter, E., Walder-Rohner, L., Haas, H., Hundhammer, T., and Wolf, U. (2023). “A prospective observational pilot study on the effects of the activity-based stress release program on the mental state and autonomic nervous system in psychiatric patients” in Oxygen transport to tissue xliv. eds. F. Scholkmann, J. Lamanna, and U. Wolf (Cham: Springer International Publishing), 231–237.
Kriakous, S. A., Elliott, K. A., Lamers, C., and Owen, R. (2021). The effectiveness of mindfulness-based stress reduction on the psychological functioning of healthcare professionals: a systematic review. Mindfulness (N Y) 12, 1–28. doi: 10.1007/s12671-020-01500-9
Krueger, C., and Tian, L. (2004). A comparison of the general linear mixed model and repeated measures Anova using a dataset with multiple missing data points. Biol. Res. Nurs. 6, 151–157. doi: 10.1177/1099800404267682
Lagraauw, H. M., Kuiper, J., and Bot, I. (2015). Acute and chronic psychological stress as risk factors for cardiovascular disease: insights gained from epidemiological, clinical and experimental studies. Brain Behav. Immun. 50, 18–30. doi: 10.1016/j.bbi.2015.08.007
Lamothe, M., Rondeau, É., Malboeuf-Hurtubise, C., Duval, M., and Sultan, S. (2016). Outcomes of Mbsr or Mbsr-based interventions in health care providers: a systematic review with a focus on empathy and emotional competencies. Complement. Ther. Med. 24, 19–28. doi: 10.1016/j.ctim.2015.11.001
Lampe, L. C., and Müller-Hilke, B. (2021). Mindfulness-based intervention helps preclinical medical students to contain stress, maintain mindfulness and improve academic success. BMC Med. Educ. 21:145. doi: 10.1186/s12909-021-02578-y
Lavrencic, L. M., Donovan, T., Moffatt, L., Keiller, T., Allan, W., Delbaere, K., et al. (2021). Ngarraanga Giinganay (‘thinking peacefully’): co-design and pilot study of a culturally-grounded mindfulness-based stress reduction program with older first nations Australians. Eval. Program Plann. 87:101929. doi: 10.1016/j.evalprogplan.2021.101929
Lee, J., Kim, K. H., Webster, C. S., and Henning, M. A. (2021). The evolution of mindfulness from 1916 to 2019. Mindfulness 12, 1849–1859. doi: 10.1007/s12671-021-01603-x
Lloyd, A., White, R., Eames, C., and Crane, R. (2018). The utility of home-practice in mindfulness-based group interventions: a systematic review. Mindfulness 9, 673–692. doi: 10.1007/s12671-017-0813-z
Mackillop, J., and Anderson, E. J. (2007). Further psychometric validation of the mindful attention awareness scale (Maas). J. Psychopathol. Behav. Assess. 29, 289–293. doi: 10.1007/s10862-007-9045-1
Mamtani, R., and Mamtani, R. (2005). Ayurveda and yoga in cardiovascular diseases. Cardiol. Rev. 13, 155–162.
Mcewen, B. S., and Morrison, J. H. (2013). The brain on stress: vulnerability and plasticity of the prefrontal cortex over the life course. Neuron 79, 16–29. doi: 10.1016/j.neuron.2013.06.028
Meaden, J. (2024). The environmental model of mindfulness. Front. Soc. Psychol. 2:1385819. doi: 10.3389/frsps.2024.1385819
Meyerowitz-Katz, G., Ravi, S., Arnolda, L., Feng, X., Maberly, G., and Astell-Burt, T. (2020). Rates of attrition and dropout in app-based interventions for chronic disease: systematic review and Meta-analysis. J. Med. Internet Res. 22:e20283. doi: 10.2196/20283
Michalak, J., Heidenreich, T., Ströhle, G., and Nachtigall, C. (2008). Die deutsche version der mindful attention and awareness scale (maas) psychometrische befunde zu einem achtsamkeitsfragebogen. Z. Klin. Psychol. Psychother. 37, 200–208. doi: 10.1026/1616-3443.37.3.200
Mishra, P., Singh, U., Pandey, C. M., Mishra, P., and Pandey, G. (2019). Application of student's t-test, analysis of variance, and covariance. Ann. Card. Anaesth. 22, 407–411. doi: 10.4103/aca.ACA_94_19
Mrazek, A. J., Mrazek, M. D., Cherolini, C. M., Cloughesy, J. N., Cynman, D. J., Gougis, L. J., et al. (2019). The future of mindfulness training is digital, and the future is now. Curr. Opin. Psychol. 28, 81–86. doi: 10.1016/j.copsyc.2018.11.012
Norouzian, R., and Plonsky, L. (2018). Eta- and partial eta-squared in L2 research: a cautionary review and guide to more appropriate usage. Second. Lang. Res. 34, 257–271. doi: 10.1177/0267658316684904
Nyklíček, I., and Kuijpers, K. F. (2008). Effects of mindfulness-based stress reduction intervention on psychological well-being and quality of life: is increased mindfulness indeed the mechanism? Ann. Behav. Med. 35, 331–340. doi: 10.1007/s12160-008-9030-2
Özcan, D., and Karapapak, M. (2024). Effect of mindfulness-based stress reduction on acute central serous chorioretinopathy: a randomized control trial. Int. Ophthalmol. 44:183. doi: 10.1007/s10792-024-03102-z
Parsons, C. E., Crane, C., Parsons, L. J., Fjorback, L. O., and Kuyken, W. (2017). Home practice in mindfulness-based cognitive therapy and mindfulness-based stress reduction: a systematic review and meta-analysis of participants' mindfulness practice and its association with outcomes. Behav. Res. Ther. 95, 29–41. doi: 10.1016/j.brat.2017.05.004
Petersen, M., and La Cour, P. (2016). Mindfulness—what works for whom? Referral, feasibility, and user perspectives regarding patients with mixed chronic pain. J. Altern. Complement. Med. 22, 298–305. doi: 10.1089/acm.2015.0310
Pinheiro, J., and Bates, D.R Core Team (2023). _nlme: linear and nonlinear mixed effects models_. R Package Version 3.1-164.
Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 6, 135–147. doi: 10.1016/j.edurev.2010.12.001
Rostaminezhad, M., Mozayani, N., Norozi, D., and Iziy, M. (2013). Factors related to e-learner dropout: case study of Iust elearning center. Procedia Soc. Behav. Sci. 83, 522–527. doi: 10.1016/j.sbspro.2013.06.100
Salmon, P., Lush, E., Jablonski, M., and Sephton, S. E. (2009). Yoga and mindfulness: clinical aspects of an ancient mind/body practice. Cogn. Behav. Pract. 16, 59–72. doi: 10.1016/j.cbpra.2008.07.002
Sapolsky, R. M. (2007). Stress, stress-related disease, and emotional regulation. Handbook of emotion regulation. New York, NY: The Guilford Press.
Segal, Z., Williams, M., and Teasdale, J. (2018). Mindfulness-based cognitive therapy for depression : Guilford Publications.
Shapiro, S. L., Astin, J. A., Bishop, S. R., and Cordova, M. (2005). Mindfulness-based stress reduction for health care professionals: results from a randomized trial. Int. J. Stress. Manag. 12, 164–176. doi: 10.1037/1072-5245.12.2.164
Shapiro, S. L., Brown, K. W., Thoresen, C., and Plante, T. G. (2011). The moderation of mindfulness-based stress reduction effects by trait mindfulness: results from a randomized controlled trial. J. Clin. Psychol. 67, 267–277. doi: 10.1002/jclp.20761
Sinha, R., and Jastreboff, A. M. (2013). Stress as a common risk factor for obesity and addiction. Biol. Psychiatry 73, 827–835. doi: 10.1016/j.biopsych.2013.01.032
Smithers-Sheedy, H., Waight, E., Swinburn, K. L., Given, F., Hooke, K., Webb, A., et al. (2024). Evaluation of a modified mindfulness-based stress reduction intervention for adults with cerebral palsy and anxiety and/or emotion regulation difficulties—A randomised control trial. J. Clin. Med. 13:1. doi: 10.3390/jcm13010001
Sommers-Spijkerman, M., Austin, J., Bohlmeijer, E., and Pots, W. (2021). New evidence in the booming field of online mindfulness: an updated Meta-analysis of randomized controlled trials. JMIR Ment. Health 8:e28168. doi: 10.2196/28168
Spijkerman, M. P. J., Pots, W. T. M., and Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: a review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 45, 102–114. doi: 10.1016/j.cpr.2016.03.009
Steiner, R. (2009b). Nervosität und Ichheit: Stressbewältigung von Innen; ein Vortrag, gehalten in München am 11. Januar 1912 : Rudolf-Steiner-Verlag.
Steiner, R., and Dietler, U. (2006). Anthroposophie und Buddhismus: ausgewählte Texte : Rudolf-Steiner-Verlag.
Tang, R., and Braver, T. S. (2020). Predicting individual preferences in mindfulness techniques using personality traits. Front. Psychol. 11:1163. doi: 10.3389/fpsyg.2020.01163
Teo, J. L., Bird, S. R., Wang, X., and Zheng, Z. (2024). Using telehealth to deliver qi gong and tai chi programs: a mixed-methods systematic review on feasibility, acceptability and participant engagement factors. Arch. Gerontol. Geriatr. 117:105203. doi: 10.1016/j.archger.2023.105203
Ungunmerr, M.-R. (2017). To be listened to in her teaching: Dadirri: inner deep listening and quiet still awareness. EarthSong J. 3, 14–15.
Vanitallie, T. B. (2002). Stress: a risk factor for serious illness. Metab. Clin. Exp. 51, 40–45. doi: 10.1053/meta.2002.33191
Yu, J., Han, M., Miao, F., and Hua, D. (2023). Using mindfulness-based stress reduction to relieve loneliness, anxiety, and depression in cancer patients: a systematic review and meta-analysis. Medicine (Baltimore) 102:e34917. doi: 10.1097/MD.0000000000034917
0 comments
Leave a comment
Please log in or register to post a comment